assessment
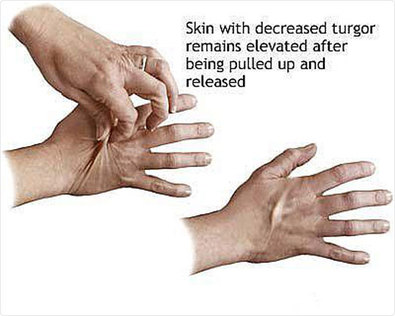
- Assess skin elasticity
- Assess for sunken eyes
- Assess for severely reduced urine output
- Pinch skin and assess how fast or slow it springs back,
- Assess for dry areas around the mouth and nose
- Assess for low breathing patterns
- Assess for lack of tears in eyes
- Assess for watery, loose stool
nursing diagnosis
- Loss of fluid volume related to low fluid intake as evidence by nausea

plan
- By March 2nd 2014 patient will have maintained appropriate fluid volume with good skin elasticity and no swelling. Patient will urinate 30 ml/hour. Stool will be solid, formed and brown in color.

intervention
- Increase fluid intake to 2500 ml/day to increase amount of fluid in body
- Cover the patient with light sheets while in bed to promote comfort and avoid overheating to prevent fluid loss
- Provide patient with container with marked measurements to urinate in to properly keep track of how much they are urinating and the color of the urine
- Assess or instruct patient to monitor weight daily and consistently, with same scale, and preferably at the same time of day
- Monitor active fluid loss from wound drainage, tubes, diarrhea, bleeding, and vomiting; maintain accurate input and output.
- Evaluate fluid status in relation to dietary intake. Determine if patient has been on a fluid restriction.
evaluation
- By following Nursing Interventions, patient has reached normal fluid volume. Patient’s skin elasticity has returned. Areas around mouth and nose are moist. Stool is formed, solid and brown in color. Patient is urinating 30ml/hour. Patient has no signs of swelling.
